
Prostate Cancer can be very difficult to detect. Deciding what to do about it if we find or suspect it can be even tougher, for patients and their physicians. Of course, we want to treat aggressive, potentially lethal prostate tumors. But we don’t want patients to endure needless worry and undergo unwarranted medical procedures if their cancer is slow-growing and not life-threatening.
The existing methods we’ve used to look for prostate cancer haven’t improved much in the last three decades. The traditional digital rectal exam isn’t a very effective screening tool; probing with a finger can only access part of the gland, so we may miss some cancers. And by the time tumors grow large enough to be felt with the finger exam, they may be at an advanced stage.
The prostate specific antigen (PSA) blood test, since 1994 a companion to the digital rectal exam for screening older men, measures levels of a protein that often go up when prostate cancer is present. But other conditions besides cancer can elevate PSA levels. And there’s no clear-cut “normal” PSA level. Many men with a high PSA result don’t actually have prostate cancer, while some with low levels do.
If repeatedly worrisome PSA results point to the possibility of prostate cancer, we turn to a prostate biopsy to confirm the diagnosis. But like the digital rectal exam and the PSA test, this tool has limitations.
To obtain prostate tissue for cancer testing, we poke a series of needles (between 12 and 24) into different areas of the gland, guided by ultrasound. We’ve used this method since the 1980s. The ultrasound images help us place the needles properly, but the pictures aren’t distinct enough for us to be able to tell cancerous from normal prostate tissue, so we can’t target and hone in on suspicious areas for biopsy. We’re using a scattershot “blind” approach, hoping that, if a tumor is present, one of the needles will encounter it.
The healthcare providers at East Valley Urology Center now offer a newer, more advanced technology to help improve the accuracy of prostate cancer biopsies. Fusion guided biopsy, which most health insurance plans cover, is a welcomed addition to our arsenal of cancer-fighting tools. This approach allows our providers to ensure they sample suspicious sites in the prostate where there is a concern for cancer. Let me explain why it’s needed and how it works.
Recently, researchers have developed software that “fuses” detailed MRI scans with live, real-time ultrasound images of the prostate. A patient first undergoes a 3T MRI scan of the prostate. Subsequently, a radiologist will analyze the images and help create a three dimensional image of the prostate, indicating abnormal areas or suspicious lesions, marking these spots on the images.
Later, the patient will undergo the procedure in our office under anesthetic. We insert an ultrasound probe into the patient’s rectum. As we move the probe around the prostate, the fusion software shifts the overlaid MRI image accordingly, giving us a detailed 3-D ultrasound/MRI view. We can use the fused image to guide the biopsy needles precisely to the lesion we want to sample rather than poking around and hoping we find something. It’s like using a GPS to reach your destination rather than driving without directions.
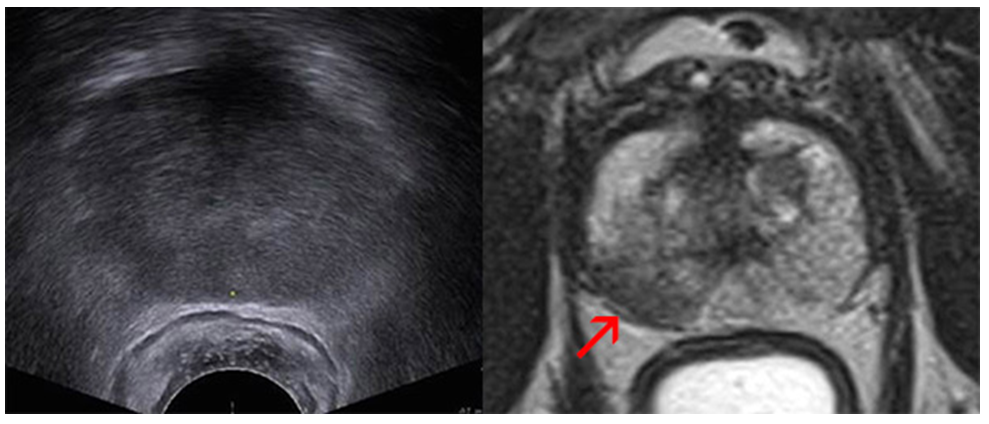
As you can see in these images, an MRI scan (right) provides much more detail of the prostate than an ultrasound scan (left) does, showing a dark area (arrow) that suggests a tumor.
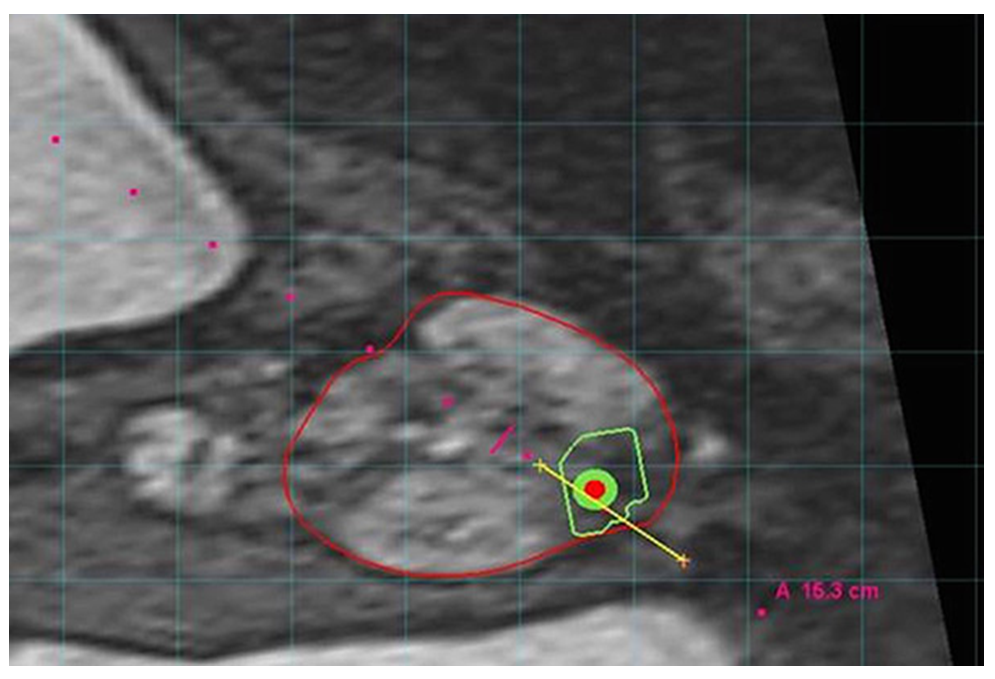
When the MRI and ultrasound images are fused, we get an even clearer target to biopsy. Below is the fusion guided image we see during the biopsy procedure, with the prostate outlined in red, the suspected tumor in green and the biopsy needle in yellow.
What are the benefits of the MRI fusion biopsy?
You may be a candidate for this procedure if you have:
The MRI Fusion Biopsy is not perfect.
Please remember, the fusion guided biopsy approach isn’t perfect. A recent study found that the fusion method may miss many prostate tumors just like the standard biopsy. But the cancers that the fusion method misses are far more likely to be clinically insignificant. Put another way, fusion guided biopsy is better than the existing approach at finding prostate tumors we need to treat, while overlooking those we don’t need to worry about.
Preparation for the biopsy
You cannot take aspirin or other blood thinners, such as Plavix, Eliquis, Brilinta, Pradaxa, Coumadin, Warfarin, Ibuprofen, Naproxen, Aleve, Advil, Celebrex, Ecotrin, and many others for several days prior to your scheduled biopsy. If you take any of these or other anticoagulants please discuss this with our scheduler. It might be necessary that you also consult with your Cardiologist prior to stopping.
The day before the biopsy
The night before your exam, you need to take an antibiotic as prescribed by your physician before going to bed. If you have not received any prescription for an antibiotic please contact our office immediately.
The day of the biopsy
The morning of the exam, give yourself a Fleet enema two hours before your biopsy, which is available over the counter and follow the instructions on the packaging. The enema helps to clean out the rectum and to minimize the risk of infection.
You should take your usual medications, except for the above-mentioned blood thinners if applicable.
If you have undergone a recent artificial joint replacement (<6 months ago) you might need to take additional antibiotics about 1-2 hours prior to the biopsy. Please notify the office if you have a recent history of such procedure, or if you usually take antibiotics before e.g. dental procedures.
After your biopsy
Please be sure to finish your antibiotics as prescribed. If you did not receive office anesthesia, there are no restrictions on driving after the procedure. If you received office anesthesia, you must have a driver available.
Biopsy results are typically available in 5-7 days. Your ordering healthcare provider will be notified of the results, who will then share them with you at your follow up appointment or by phone.
Possible side effects from the biopsy
Hematuria (blood in the urine) is the most common complication after prostate biopsy (20 to 63%), is usually only very slight, and subsides usually completely after a couple of days.
Hematochezia (blood per rectum) is common as well, and seen in 2% to 22% of patients. Typically, rectal bleeding is minor and easily controllable with the ultrasound probe or digitally applied pressure at the conclusion of the biopsy; rarely, persistent bleeding may require proctoscopic assessment.
Hematospermia (blood in the ejaculate) is of minor clinical concern and is found in up to 50% of men after their biopsy. It may persist for several months after prostate biopsy.
Most infectious complications after biopsy are limited to simple urinary tract infections and low-grade fever, which can be readily treated with antibiotics. With the routine use of antibiotic prophylaxis as described above 2% of patients will develop a febrile urinary tract infection, bacteremia, epididymitis or acute prostatitis that may require hospitalization for i.v. antibiotics.
Acute urinary retention requiring temporary intraurethral catheter placement occurs in up to 0.4%; mostly men with an enlarged prostate (BPH) at baseline are at increased risk.